
Completely oblivious of the implications of her body’s positioning, Rebecca Branagan, 30, reportedly began a lifetime of chronic knee pain by sitting awkwardly for two minutes Tuesday. According to sources, Branagan’s slight five millimeter shift of bodyweight while her knee was folded oddly underneath her for a little over a minute caused irreparable damage to the ligaments that would plague her for the next four or five decades. Several reports confirmed that the suffering triggered by the brief unnatural positioning that would force her to try multiple pain medications to alleviate the agonizing spasms she would get from the moment she woke up until she went to sleep at night would never go away and more likely only worsen until the day she died. At press time, Branagan had stood up from the weird position and started stretching and shaking out her legs to get the strange feeling in her knee to go away.
https://www.theonion.com/knee-to-hurt-for-rest-of-life-after-30-year-old-woman-s-1847055269
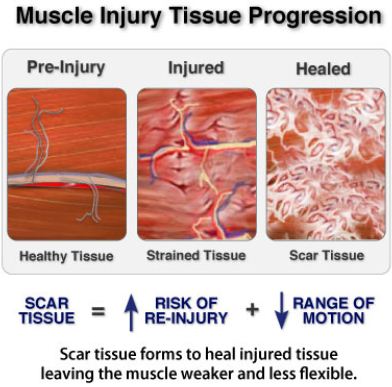
While The Onion is usually satire, the article is not far from the truth. While the injury of a strained ligament or torn cartilage may not be curable - to the extent that it never happened. Medication may provide some relief but will not cure the problem. Surgery may eventualy be necessary but it will not restore the tissue to new and can often muck things up worse. The goal of therapy would be to stabiize the injury and then maintain it.























 RSS Feed
RSS Feed


